

As of this writing, diabetes mellitus remains
a major global health threat. The International Diabetes Federation (IDF)
estimates that one
in 11 — or a little over nine percent — of the world's population is
affected by this disease. Moreover, that number is expected to go up to 10
percent by 2040.
Of the world's adult diabetics, 37 percent
are located in the Western Pacific region — composed of 37 countries including Japan,
China, and Australia. Meanwhile, one in eight adults in North America and the
Caribbean are diabetic; Europe has the highest number of children with type one
diabetes, and two-thirds of Africa's diabetics remain undiagnosed.
These are worrisome statistics, but not just
because they show how widespread the disease is. Recent studies suggest that
diabetes might be linked to a rarer, but arguably deadlier, condition: tuberculosis.
How
Diabetes May Increase Tuberculosis Risk
 In Chennai, India, researchers studied 209
patients with pulmonary tuberculosis. Of these, 54.1
percent had diabetes, while 21 percent were at risk of developing the same.
This is a significant jump from previous estimates, which estimated that 25
percent of tuberculosis patients also suffered from diabetes.
In Chennai, India, researchers studied 209
patients with pulmonary tuberculosis. Of these, 54.1
percent had diabetes, while 21 percent were at risk of developing the same.
This is a significant jump from previous estimates, which estimated that 25
percent of tuberculosis patients also suffered from diabetes.
Granted the aforementioned study is still
in the preliminary stage. There's a possibility the relationship between tuberculosis
and diabetes is correlative but not causative. However, a study by Dr. Bianca
I. Restrepo of the University of Texas' Health Science Center suggests it may
be the latter.
In a paper presented to the 2013
World Diabetes Congress, Restrepo expanded on studies which found a
positive relationship between the two. Since those studies based their data on
patients who already had full-blown tuberculosis, they don't answer one
question: "If a patient only had latent tuberculosis before, and became
pre-diabetic later, would the latter necessarily aggravate the former?"
Based on their findings, the answer is
"yes." After analyzing patients from the Texas-Mexico border, they
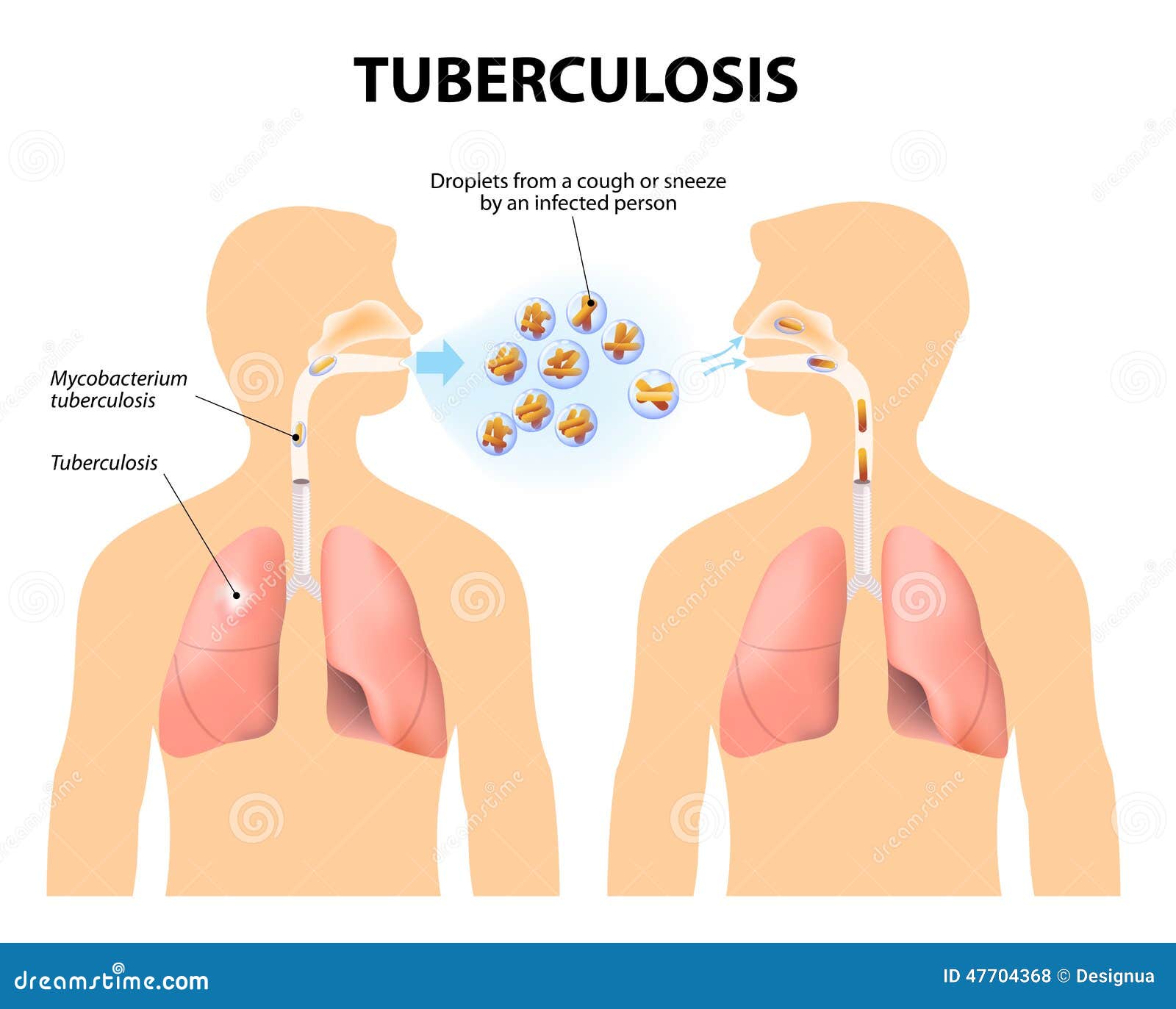
found that diabetes — specifically, type two diabetes — lowered the body's immune
response against Mycobacterium
tuberculosis (MTB). However, as
Restrepo cautions, the efficiency of the response given in the scenario above remains
unclear, so further studies on the subject are necessary.
What
Has Been Done
Since the relationship between diabetes and
tuberculosis has been established, two-prong programs have been set up around
the world. For example, the "Directly Observed Treatment,
Short-course" (DOTS) program was implemented in Angola, where 474
per 100,000 individuals develop tuberculosis.
Financed by the World Diabetes Foundation,
the DOTS program aims not only to educate patients on tuberculosis, but also to
ensure that they take the right drugs in the prescribed manner. The DOTS also
monitors patients until the end of their treatment.

Likewise, during the 2013 World Diabetes
Congress, Dr. Richard Brostrom mentioned similar initiatives implemented in the
Pacific region. They're all based on a set of "standards for management of
tuberculosis and diabetes," which Brostrom and his team have executed with
a great degree of success.
In addition to these large-scale programs, the
medical realm holds promising developments. In 2015, researchers proposed a five-year
study to analyze whether bacilli Calmette-Guerin (BCG) — the standard vaccine
for tuberculosis — may also be
used to treat type one diabetes.
Essentially, BCG stimulates the production
of tumor necrosis factor (TNF) in the body. The TNF, in turn, reduces the
diabetic immune system's tendency to attack insulin-producing beta cells, while
simultaneously encouraging the production of "good" immune system
cells.
What
Still Needs to Be Done
The scientific community still has a long
way to go. Some have doubts regarding the BCG vaccine. As Dr. Joel Zonszein,
director of Montefiore Medical Center's clinical diabetes center, points out, the
idea that selective immunosuppression works against diabetes is up for debate. It's
a step in the right direction, but it's not yet a cure by any means.
Also, there have been difficulties with the
implementation of certain TB-DM (tuberculosis-diabetes mellitus) programs. Dr.
Brostrom mentioned several plans, like the profiling of DM patients according
to their TB risk and TB screening guidance, which are still works-in-progress. The
sooner these plans are refined and implemented, the more patients will be
treated, and the more lives can be saved.
 Takeaways
Takeaways
It's important to stress that diabetes does
not directly cause tuberculosis. Rather, the former is a contributing factor to
the latter — but a significant one.
Considering the prevalence of diabetes, and
the global mobility of the human race in general, it's safe to assume
tuberculosis may find its way back to developed countries once again. When this
happens, there's no guarantee everyone can fight against two potentially-fatal
diseases at the same time.
Luckily, humanity still has hope. If the
scientific community is willing to dig deeper into the TB-DM relationship and
to implement more initiatives to combat one or the other, the worst-case
scenario may not happen after all. As Michel Sidibe, UNAIDS executive director,
once quipped: "When a virus and a bacteria can work so well together — why
can't we?"
Megan
Ray Nichols enjoys writing about various topics in health. Now that you’ve
learned a bit about tuberculosis, you might like to learn more about mental health.
No comments:
Post a Comment
Pharmaceutical Microbiology Resources