As a prototype for the future, is it possible to consider an energy
efficient filter system that cost-effectively maintains airflow towards a
reduced rate of change? Michael Rodd, Chief Sales Officer at M+W Products (www.products.mwgroup.net) looks at elements of life sciences in the
clean room and envisages how future practice can radically change the concept
of clean room procedures.
It is common to expect the output
of a clean room operation to end as a microprocessor in your phone, laptop or
car, but in fact, the first measured effort to control an environment was used
for medicinal purposes on a table in a hospital. British surgeon Joseph Lister
in 1867, at a time when multiple surgeries were performed using the same
contaminated equipment, sterilised his hand using carbolic acid and
experimented implementing this technique on wounds and needles to discover the
elimination of bacteria.
Although much has changed since,
and both our efforts and realisations of scientific procedures have adapted,
the dedication of modern life sciences was reinvigor
ated as
a fairly new discipline of the clean room subdivision over the last century. This
process encapsulates everything utilised by the way of clean room technologies
in the production of medical substances, pharmaceuticals and biological
compounds.

As the history of the pharma
world displays, our requirement for a clean room stems from the need for
contamination control. Whether that’s using gloves during primitive operations
or alcohol as an antiseptic to sterilise needles or creating paint and lacquer
work out in uncontaminated air near the Pacific Ocean, our need to benefit from
such processes has been fuelled by the requirement to control and clean our
imminent environment.
This demonstrates something else
too – that the clean room has developed from a permutation of science and
engineering – assessing scientific processes that have worked and engineering
them to deliver better results. This multidisciplinary approach has been
encased by technological practices available at certain periods of time.

Fundamental to the field of life
sciences and pharmaceutical micro biotechnology is contamination control. First
and foremost, the apparatus used for pharmaceuticals in clean room laboratories
should be dedicated and separated from other areas. Nailed down, this involves
the classification between protecting the working environment and protecting
the operator from any potential contamination. This is because humans remain
the biggest cause of contamination; that may never change. To put this into
perspective, the outer layer of human skin can host up to 1 million
microorganisms per square cm, and equally, human saliva up to 1 billion per
square ml.
The frenzy of microbes is
difficult to keep on top of at every stage of the process. Basic negligence can
cause the microorganisms from our clothes, mobile phones or bare skin to
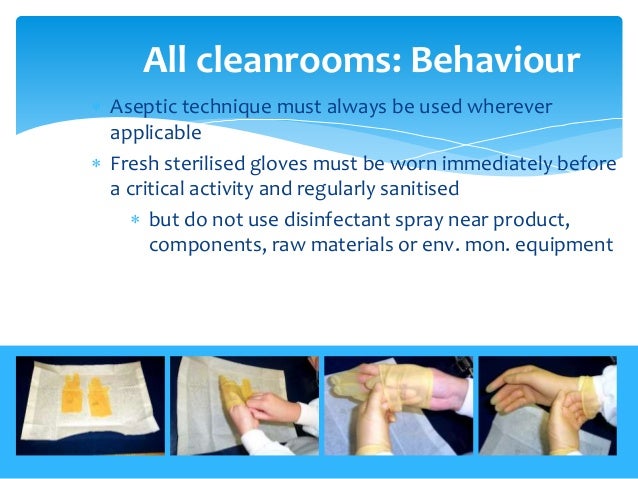
contaminate working stations. For instance, hands, whether gloved or un-gloved,
are one of the main sources of spreading infection or transferring microbial
contamination. Thus, an important part of good contamination control within a
cleanroom requires the use of cleaning and disinfection agents. It goes without
saying that just as personnel may be the biggest contaminants, they are also
critical to the maintenance of
asepsis in a controlled environment.
Therefore diligence and training in clean room technology is essential
throughout the entire process.
The improper analysis of
microbiological inspections may cause inadvertent contamination. Therefore, thorough
aseptic processing like product or microbial bioburden to calculate viable
organisms is needed to prevent any sort of contamination during the process
stream. In some cases, even measuring total particulate count within a vessel
does not cater for the continuous generation of organisms by individuals;
therefore it does not always quantitate all contaminants and provide the whole
picture of microbiological content. Microorganisms will associate with physical
particulates and therefore it is necessary to include monitoring techniques
that satisfy both the classification and regulatory requirements by
differentiating the microbiological components of an operation. Stringent
optimisation of tests will give assurance that bioburden of the environment is
apt for clean laboratory practices.
In its simplest form, a product
being operated within a clean room during a process line includes an enclosed
vessel or large container that is sealed from external air temperature.
Throughout this process, it is the aim of every operative to maintain
conditions to a level where they can be declared sterile or aseptic.

A clean room is classified based
on the cleanliness of its air so as far as clean rooms go, anyone wants to keep
the environment as clean as possible. One of the trends we’ve seen across this
spectrum (and it is a large spectrum) is on the lower end quality scale
concerned with areas that are
Clean Not
Classified (CNC). These are areas that can be regarded
clean within definitive purposes of the word in regards to the
production area, but they are not actually
classified
because they work on a process we call Good Manufacturing Practice (GMP) or
Current Good Manufacturing Practice (CGMP).
The ability to manufacture
medical devices with consistent high quality relies on well implemented and
well documented GMP. The GMP code sets out a guideline to achieve sterility
assurance. Any business that delivers clean room technology requires constant
monitoring and up-to-date certification.
The measurement most universally
applied is the Grade A-D standard, whereby a cubic foot sample is taken of the
environment and the number of particles greater than 0.5mm measured within
it. Areas are classified on a graded
system from A onwards, with A being the cleanest.
So the purpose of a low quality CNC is to effectively get as close as possible
to classification. D certified environments accept the inclusion of certain
particles even in dynamic conditions (i.e. when people are operating within
contained vessels) with turbulent airflow, whereas A certified environments
deal with linear laminated airflow that is non-turbulent. Cleanliness is
commonly achieved through the development of effective HEPA (High Efficiency
Particulate Air) filtration and this is considered as clean as necessary for a
GMP Grade A condition.

Let’s complicate things a step
further. Introduced here is the onion concept. Its name is derived from the idea
that as you peel the onion, a processor must past through successive cleaner
areas to reach the centre, non-turbulent, Grade A area. In essence, the onion
concept caters for the disposal of multiple grade conditions within the same
vessel or container.

Furthermore, the application of
disinfectants on specimens reduces the microbial bioburden as we discussed
earlier. Therefore, when collecting environmental monitoring samples, personnel
should begin with Grade A locations and then move on to areas that are away
from technical apparatus but still within the controlled zone.
This grade system is applicable
in cases where processors and products are exposed during transportation, or
operations that are required to be performed outside of sealed compartments.
Grade B is commonly of high purity but does not necessarily involve laminate
air flow. So the trick here lies in maintaining airflow to a certain speed. Essentially,
imagine the onion concept: each time a layer of the onion is peeled, the amount
of particulate or contaminated risk to the product is reduced.
 For any sales or financial
operative, however, this all costs money and clean rooms are an expensive
market already. The integration of new technology and efficient solutions has
ignited consideration of future controlled environmental procedures to limit
the number of air changes per hour. Can future systems be both more efficient and
challenge the tradition of multiple air changes and still ensure constant clean
air? This is a radical thought and not on the agenda yet, but with a global
drive for efficiency and cost-saving mechanics already found within homes and
our cars, is there a need for such ideas to be infused as part of the life
science debate? A future model to strive for would be to find an energy
efficient procedure of controlled environments that maintains the right quality
and temperature at the lowest price possible. The future of pharmaceutical
trends in the clean room is exciting.
For any sales or financial
operative, however, this all costs money and clean rooms are an expensive
market already. The integration of new technology and efficient solutions has
ignited consideration of future controlled environmental procedures to limit
the number of air changes per hour. Can future systems be both more efficient and
challenge the tradition of multiple air changes and still ensure constant clean
air? This is a radical thought and not on the agenda yet, but with a global
drive for efficiency and cost-saving mechanics already found within homes and
our cars, is there a need for such ideas to be infused as part of the life
science debate? A future model to strive for would be to find an energy
efficient procedure of controlled environments that maintains the right quality
and temperature at the lowest price possible. The future of pharmaceutical
trends in the clean room is exciting.









 The human intestines are home to trillions of microorganisms (many bacteria, some fungi, and by-products – collectively known as the microbiome). Several strands of research are showing how the numbers and types of certain bacteria are important for the regulation of immune function and how disruption can lead to autoimmune diseases.
The human intestines are home to trillions of microorganisms (many bacteria, some fungi, and by-products – collectively known as the microbiome). Several strands of research are showing how the numbers and types of certain bacteria are important for the regulation of immune function and how disruption can lead to autoimmune diseases.




 Scientists from the National Physical Laboratory (NPL) and
University College London (UCL) have converted a breast milk protein into an
artificial virus that kills bacteria on contact.
Scientists from the National Physical Laboratory (NPL) and
University College London (UCL) have converted a breast milk protein into an
artificial virus that kills bacteria on contact.
 During the last 20 years, overuse of antibiotics has helped to create drug-resistant strains of the bacterium that have turned tuberculosis from a Victorian-era disease that was often romanticized into something that needs to be feared and respected once again.
During the last 20 years, overuse of antibiotics has helped to create drug-resistant strains of the bacterium that have turned tuberculosis from a Victorian-era disease that was often romanticized into something that needs to be feared and respected once again. 
 While there is a great call right now for countries to open their borders in the wake of the events in Syria that left many as refugees, the borders should be opened intelligently.
While there is a great call right now for countries to open their borders in the wake of the events in Syria that left many as refugees, the borders should be opened intelligently.